
Tools of the Trade
Temporary Particulates
Gelfoam – water-soluble agent derived from purified skin gelatin. Vessel tends to recanalize in a 3 wks - 3 mo. Very versatile from intravascular embolization to embolization of biopsy tracks in solid organs to reduce bleeding risks.
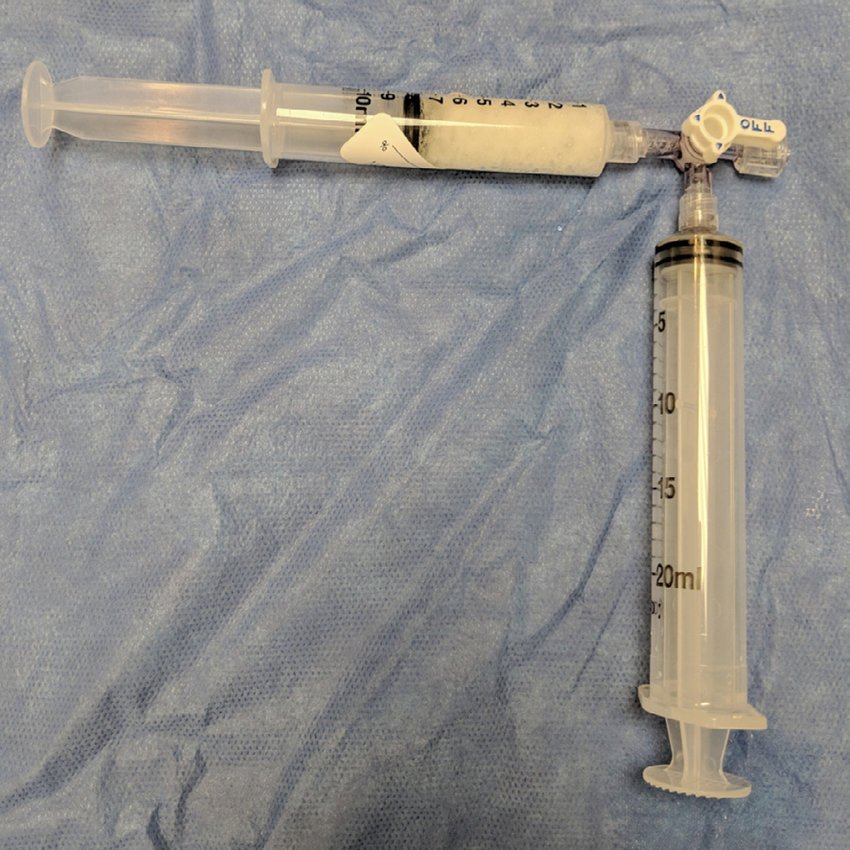
Slurry, torpedos, and pledgets - Gelfoam comes in small foam sheets (B in the left image below). It can be made into a slurry by cutting it into small pieces and suspending in saline flushing back and forth between two syringes as shown in the images below. It can also be cut and rolled into little cylinders to either be precisely unsheathed in a percutaneous tract (“pledget”) or injected (“torpedo”).
EmboCube (Merit) - Uniformly pre-cut gelatin foam in syringes
Merit Torpedo - Pre-made gelfoam cylinders that can be used as pledgets or torpedos

Lipiodol (Guerbet) - iodinated poppy seed ethyl esters, viscosity similar to blood
WARNING: Use cautiously if sensitive to iodine, e.g., allergy or thyroid disease
An advantage of lipiodol is that it can stain a target tumor, e.g., prior to ablation or used in combination with chemotherapeutic agents for chemoembolization
Guerbet now make syringes and 3-ways resistant to being dissolved by lipiodol
Avitene – microfiber collagen powder; can be used through a microcatheter. Moderate recanalization in 2 weeks, completely in 2 months
Permanent Particulates
Polyvinyl Alcohol (PVA) – irregularly shaped shavings 50-1200 um or microspheres. Has a tendency to clump more than microspheres but has the best data for things like UFE.
Microspheres – easier to inject with less catheter clogging and clumping. Tend to come in premade syringes with set range of particle size, e.g., 300-500 um. Beads can be bland or loaded with medication such as for chemoembolization.
Embozene (Varian) - more tightly calibrate, syringes come in a set particle size, e.g., 500 um
Embosphere (Merit) - less tightly calibrated, syringes come in a range of particle sizes, e.g, 500-700 um
Others include Hydropearl (Terumo)
Permanent Mechanical
Coils – requires functional platelets. Generally need to oversize ~20-30% for arteries or more for veins to prevent dislodgement. Coils vary is size, length, stiffness, and other qualities such as having fibers to stimulate thrombosis.
Framing vs Packing coils - Stiffer framing coils with more radial force are placed first to provide scaffolding for softer packing coils used to more tightly pack the vessel, aneurysm, etc.
Pushable vs Detachable coils - Pushable coils cannot be retracted once pushed or injected out of a catheter whereas Detachable coils can be retracted back into the catheter prior to detachment. Detachable coils are good for tenuous areas where very precise placement is necessary but tend to cost substantially more.
Some coils have thrombogeic fibers attached. Others are coated with hydrogel that expands after deployment to aid with vessel occlusion.
Vascular Plugs (e.g. Abbott Amplatzer plugs) – tight nitinol mesh ideal for single-step occlusion. Tend to oversize 30-50% per manufacturer. Often more expensive than coils but can save time and cost if the embolization would otherwise require many coils.
Balloons – no longer available in U.S. due to placement accuracy difficulty
Permanent Liquids (good if coagulopathic)
Glue (N-butyl cyanoacrylate) – rapid polymerization upon contact with ionic substance (e.g. plasma, saline). Can rapidly solidify in catheter so catheter is first flushed with nonionic D5W. Tends to be more inflammatory than particle embolic agents.
Histoacryl <<<< Trufill in terms of cost
Glue is mixed with anionic contrast agent to visualize such as lipiodol in a 1:1 to 1:9 ratio to adjust the “thickness” or how rapidly it polimerizes.
Learn more about glue embolization with Dr. Ziv Haskal on BackTable
Onyx (Medtronic) – ethylene vinyl alcohol copolymer dissolved in dimethyl sulfate (6.0, 6.5, or 8.0%; branded as Onyx 18/20/34) and opacified with tantalum. Contact with water causes DMSO to diffuse away and polymer precipitation
Pros: supposed to be cohesive rather than adhesive so theoretically less catheter sticking, slowly flowing, more controlled relative to glue
Cons: very expensive, requires DMSO-compatible catheter with risk of DMSO toxicity, time a long time to suspend, some feel the catheter sticks just as often as with glue
Obsidio (Boston Scientific) - conformable embolic that come pre-packaged in 1 cc syringes. It does not require specific catheters like Onyx or LAVA but is more expensive than LAVA.
LAVA (Sirtex) - essentially rebranded Onyx but much cheaper and the first liquid embolic to be FDA approved for peripheral embolization, e.g., bleeding. Like onyx, the downsides are that it require DMSO which is toxic, DMSO compatible catheters, and a bit more set up.
Ethanol – denudes endothelium causing thrombus formation and fibrosis, penetrates deep into capillary beds causing complete devascularization
Very effective for vascular anomalies and end organtumor embolization (e.g. AML) but higher risk of complications such as skin/nerve necrosis and systemic toxicity (minimize by using <0.14 mL/kg over 10 min period)
Ethanolamine – ethanolamine oleate and ethiodol mixture in 5:1 or 5:2 ratio; causes thrombosis and mural necrosis and vacular wall; risk of oleic acid combining with serum proteins and causing AKI, hemolysis, hepatotoxicity, and hemoglobinuria; some give prophylactic haptoglobin pre- and post-procedure
Squid (Balt)- EVOH/DMSO like Onyx with smaller tantalum powder with longer suspension time relative to Onyx
Precipitating hydrophobic injectable liquid (PHIL, MicroVention Terumo) - also DMSO based, radiopaque from iodine, producing less streak artifact, toothpaste-like consistencies in PHIL 25/30/35
Embrace hydrogel embolic system (Instylla) - polyethylene glycol injected via duel lumen catheter with initiator causing rapid solidification via intravascular polymerization, iodine based radiopacity
Phase-Transitioning Agents. (being studied) - solute to solid transition with change in environment, e.g., ionic strength triggered chelation, thermoresponsive gels, pH-sensitive agents, shear-thinning hydrogels