
Gastrointestinal and Urinary
Indications
Acute variceal hemorrhage unresponsive to endoscopic intervention - “salvage TIPS” if for first bleed or “rescue TIPS” if recurrent bleed during same hospitalization.
Prevention of recurrent variceal bleeding for patients with cirrhosis, Child Pugh 10-13 (C) or 7-9 (B) with active bleeding at endoscopy (“pre-emptive TIPS”) or later outpatient (“elective TIPS”)
This “early” TIPS is associated with less rebleeding (3% vs 50%), time in the hospital (4 vs 15 days), and 1 year survival (86% vs 61%) compared to medical management
Recurrent ascites and/or hepatic hydrothorax refractory to medical management and repeat paracenteses.
Patients who benefit have 3 or more paracenteses in a year, MELD <18, total bilirubin <5, and no overt baseline encephalopathy
PV thrombosis (multiple complex grading systems, e.g., Yerdel grade): acute (mesenteric ischemia) vs chronic (portal HTN), cirrhosis vs non-cirrhotic, partial vs complete, malignant or benign.
Budd-Chiari syndrome
Contraindications
Absolute:
Congestive heart failure stage C or D
Severe pulmonary HTN (mean pulmonary pressure >45 mmHg)
Severe uncontrolled hepatic encephalopathy
Sepsis with bacteremia
Acute liver failure
Relative:
Untreated biliary obstruction
Uncorrectable severe coagulopathy
Challenging but possible: polycystic liver disease, PV thrombus, intrahepatic tumors
Higher risk with less data for MELD >18, CP score >13, age >75
Efficacy and alternatives
TIPS for variceal bleeding: ≥95% technical success rate with 16-19% esophageal varices rebleeding rate vs. 44-47% with endoscopic interventions and 39% with medical therapy (e.g. propranolol).
However, higher rates of encephalopathy and higher costs with TIPS vs endoscopic management (incremental cost-effectiveness of $57,003/QALY)
~36% of patients who receive a TIPS emergently for variceal bleeding die within 6 weeks, so important to discuss goals of care.
TIPS is less effective for gastric than esophageal variceal bleeding. Gastric varices are thought the bleed at lower portal pressures. As such, embolization or transvenous obliteration (e.g. BRTO) is more effective for gastric varices and can be combined with TIPS. See separate lesson.
TIPS for refractory ascites: clinical improvement in 58-62%.
Recurrent large volume paracentesis or Denver shunt: TIPS has better transplant-free survival, decreased hospital days, and better patency than Denver shunts and large volume paracenteses. However, TIPS causes more encephalopathy and no clear difference in QoL.
Proximal splenic artery embolization: Can be effective if not a TIPS candidate by decreasing portal flow without substantial splenic infarction due to collaterals.
If refractory despite no portal hypertension, consider lymphatic obstruction. There have been case series showing success with angioplasty/stenting for the lymphovenous junction.
TIPS vs anticoagulation for PVT:
Anticoagulation leads to recanalization in 55-75% at 6 mo, less effective in complete thrombosis
TIPS technically successful in 75-100%, leads to complete recanalization 57%, partial in 30%, no change in 13%; worse outcomes if chronic/complete occlusion/cavernoma
Direct intrahepatic portocaval shunt (DIPS), Transjugular transcaval intragepatic portosystemic shunt (TTIPS), Mesocaval shunt:
Uncommon alternatives if anatomy is unfavorable for TIPS. Ideally the shunt of DIPS and TTIPS remains intrahepatic with ICE or transabdominal ultrasound guidance.
Can place a snare in the intrahepatic IVC and. gain percutaneous access under US-guidance through the intrahepatic RPV and to the snare in the IVC. A wire is passed allowing access. Track plasty followed by access into the MPV. The percutaneous track is then embolized.
For mesocaval shunt can do bowel prep and prophylactic antibiotics and use a 22G chiba percutaneously going through bowel, etc, like thoracic duct embolization.
TIPS has also been shown to improve portal hypertensive gastropathy, refractory hepatic hydrothorax, and possibly hepatorenal syndrome.
Data is limited for TIPS for hepatopulmonary syndrome. Current data suggest most patients have short term improvement which is not sustained and followed by long term deterioration.
Polytetrafluoroethylene (PTFE) covered stents (e.g. Viatorr) have substantially superior patency than using bare metal stents for TIPS, likely because of traversing bile ducts and bile is thrombogenic. Viatorr has also been shown to be superior to Wallstents.
If refractory ascites despite no portal hypertension, consider lymphatic obstruction. There have been case reports with improvement with angiopasty or stenting of the lymphovenous junction.
Pre-procedure work up
Hepatology/Gastroenterology evaluation with CMP, CBC, PT/INR and calculation of MELD, Child-Pugh, and ALBI scores.
Medical and endoscopic management often trialed first, e.g, octreotide 25-50 ug bolus -> 25-50 ug/hr to reduce variceal bleeding.
Traditional MELD score is superior to Na-MELD for prediction of post-TIPS mortality. However, newer MELD 3.0 may also be predictive.
Higher risk of adverse outcomes with traditional MELD>18, CP B or C, Tbili >3, ALBI >-2.60 (grade 2 or 3).
Higher risk of encephalopathy with high serum creatinine or hyponatremia.
Echocardiography to evaluate right heart function. Consider cardiology consult as well if presence of heart disease.
Contrast-enhanced CT or MRI to characterize anatomy.
Pre-procedure abx: Unysyn, cefotaxime, or ceftriaxone (vancomycin or clindamycin for PCN allergy)
There are higher rates of post-TIPS hepatobiliary infections (10.9% vs 0.4%) if the patient has a prior biliary intervention (bilioenteric anastomosis, sphincterotomy, biliary stent/drain).
Anesthesia evaluation if being done with general anesthesia, which is common
Procedure steps and tips
TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT (TIPS):
(Optional) Paracentesis. Nice to use a pigtail (e.g. 5 Fr pigtail flush catheter) and position it by the gallbladder fossa to use as a target for TIPS. Can also leave in place during the TIPS and monitor for bloody output as an early sign of bleeding complications.
Right IJ access (can use left IJ or either EJ if necessary).
If using ICE for TIPS guidance, option common femoral vein access as well. A second IJ access can work as well.
Advance stiff working wire (e.g. Amplatz) into the IVC.
Dilate access and advance sheath into right atrium (RA) +/- IVC for pressure measurement.
Consider aborting procedure if >10-12 mmHg and elective. Can try diuresis to bring down the pressure.
Select the right hepatic vein, often MPA, C2, or catheter in the kit with an angled glidewire. Middle or left hepatic vein can also be used if right is unfavorable.
Some leave the working wire in the IVC while selecting the hepatic vein.
Helpful to pull the sheath back far enough into the RA to not limit the curve of the catheter. Often the confluence of the hepatic veins and IVC is right at the inferior cavoatrial junction so may need to probe more superiorly if having trouble selecting the hepatic veins.
Confirm hepatic vein selection with venogram +/- lateral view (RHV should course posteriorly), transabdominal US, and/or ICE.
Advance sheath into hepatic vein over the wire and catheter to secure access.
(Optional) Wedge catheter and perform CO2 wedged portogram to visualize target portal vein (RPV if from RHV vs LPV if from MHV or LHV).
Confirm wedged positioning with very gentle contrast injection. Strong injection can lacerate the liver and capsule.
Some do this in two projections (AP and RAO) to help troubleshoot later. E.g. after each pass with the needle, can check AP and RAO projections to plan next attempt (e.g. not anterior enough).
Establish transhepatic portal venous access.
Access kits vary. Generally, there is a needle within a small catheter, which passes through a metal curved stiffener, which is placed through the access sheath.
Ring kit (Cook) with 16G Colapinto needle, Rosch-Uschida kit (Cook) with 21G sheath needle, Haskal kit (Cook), fine needle access kit (AngioDynamics)
Helpful to curve the metal stiffener to help target the portal vein. Advance it through the sheath a little further into the hepatic vein than intended starting point. Unsheath the metal stiffener and turn it anteriorly (for RHV to RPV) to engage the vessel wall. Then pull the stiffener back to intended starting point for pass with the needle, ideally within 2-3 cm from the ostium of the hepatic vein.
Make pass, remove needle, and aspirate slowly through catheter pulling back with syringe with dilute contrast to inject if blood return to confirm portal vein access. Ideal to hit RPV 1-2 cm from bifurcation. Too central access risks hemorrhage from extrahepatic access. Too peripheral creates an acute angulation making stent placement challenging and prone to failure.
Tips and tricks for difficult access:
Transabdominal US or ICE can be used for real-time guidance of the needle. ICE-TIPS shown to reduce procedure time, radiation, and passes.
Can opacify the portal system or pass a loop snare target if too peripheral and restick.
“Gunsight TIPS:” Obtain transhepatic portal vein access. Place a loop snare in the target portal vein and target hepatic vein. Pass long thin needle (e.g. 22G chiba) percutaneously through both snares. Pass a long 0.018” wire and remove needle. The wire can then be snared provided transhepatic access.
Catheterize portal vein - often a Bentson or glidewire advantage works well
Bentson works well because if the wire courses peripherally, it will often buckle centrally if you keep pushing. Alternatively, careful exchange for a curve catheter (e.g. C2 or RIM) can help redirect the wire into the main portal vein.
Advance 5 Fr pigtail into the portal system.
Obtain pre-TIPS portal pressure measurement through the catheter and calculate hepatic venous pressure gradient (HVPG = portal pressure - RA pressure)
Portal HTN = HVPG >5 mmHg, absolute portal pressure 22 mmHg, or splenic vein pressure of 15 mmHg
Advance pigtail catheter into the splenic vein or SMV for portal venogram. Position sheath near the hepatic vein ostium to perform simultaneous hepatic venogram.
Can attach portal catheter to power injector and perform the hepatic venogram through the sheath via hand injection once contrast is opacifying the portal system.
Can try to advance whole system with sheath into the portal vein to secure access. Alternatively, can pre-dilate after pressure measurements to 8 mm and advance sheath while deflating the balloon like a g-tube.
Measure stent length necessary for covered portion of the stent to extend from the portal vein access site to the ostium of the hepatic vein.
Viatorr endoprosthesis (Gore) is commonly used, which has 2 cm uncovered to extend into the portal system with the remainder covered. For example, is 8 cm covered stent is necessary, a “2+8 cm Viatorr” would be needed.
When in doubt, some say to add 1-2 cm or err on the side of a longer stent to account for projection overlap. Others use ICE to measure.
Advance access sheath into the main portal vein.
Can try to advance the metal stiffener with the sheath together using the curve of stiffener to measure to tract.
Alternatively, the sheath introducer can be used or pre-balloon dilation of the tract.
Advance selected stent (e.g. Viatorr) and unsheath uncovered 2 cm slightly more central in the portal system.
Pull back to engage the flared uncovered portion with the portal vein entry site prior to deploying the rest of the stent.
Carefully advance an 8 mm angioplasty balloon and dilate the stent to 8 mm to start.
Viatorr endoprostheses are designed to be adjustable from 8-10 mm.
Some studies suggest superior outcomes with dilation to 8 mm rather than 10 mm, so good to start with 8 mm or option to dilate larger if needed to decrease the HVPG.
Advance pigtail catheter back into the portal system and sheath in the RA to remeasure pressures.
Goal HVPG for variceal bleeding is <12 mmHg or 50% reduction. For refractory ascites, some studies suggest better outcomes with lower gradients, particularly <8 mmHg.
Risk of complications 35% for gradient >12 vs <5% if <12, 8.5xs the risk
If persistent HVPG elevation, the TIPS can be dilated to 10 mm. Alternatively, a parallel TIPS can be placed. Propranolol can also reduce portal pressure an additional 20-25%.
Post-TIP portal venogram.
If stent is too short, it can be extended.
(Optional) Variceal embolization
Data is mixed. Many advocate for embolization of large varices, particularly if there is persistent filling on post-TIPS venogram. There is also data suggesting benefit for gastric varices. Otherwise, some leave them alone with option to embolize later if needed.
Embolization materials vary but many use coils or plugs.
If variceal embolization is performed, repeat portal venogram and pressure measurements as embolization increases the HVPG.
Remeasure portal and RA pressure measurements via pigtail and sheath for post-stenting gradient.
Remove sheath and obtain hemostasis.
Portal Vein Recanalization TIPS (“PVR-TIPS”):
Transhepatic or transsplenic access if PVT/poorly visualized portal system (“PVR-TIPS”)
Good for Yerdel grade 2 or 3
Obtain transhepatic, transplenic and/or superior mesenteric venous access.
Transplenic access is often superior if the main portal vein is chronically thrombosed.
Access central vein to avoid tortuosity of more peripheral puncture. Can place a pigtail adjacent the spleen for ascites to help with hemostasis and watch for bloody output as sign of trouble.
Advance a 5 or 6 Fr sheath for stable access.
Advance a curved catheter and angled glidewire to catheterize the native portal veins.
Probe more cranially than you think near coronary vein to find the true lumen.
Can also try crossing catheters and ICE guidance.
Advance loop snare into the target portal vein (e.g. ideally RPV) to target for TIPS via IJ access as described above. Alternatively, can use gunsight technique described above.
Angioplasty +/- stenting of the portal system. Often just plasty for chronic occlusion as stenting can limit transplant options.
Finish placing TIPS as bove.
Embolize transhepatic/transplenic access tract carefully with gelfoam pledgets +/- coils due to high bleeding risk.
DIPS:
Similar technique to regular TIPS described above but instead direct IVC to MPV access is establish through the caudate. Often need to make a second curve in metal introducer for more of a 90* angle out of the IVC.
TIPS REVISION:
Right IJ access (can use left IJ or either EJ if necessary).
Advance stiff working wire (e.g. Amplatz) into the IVC.
Dilate access and advance long sheath (e.g. 10 Fr BriteTip) into right atrium (RA) +/- IVC for pressure measurement.
Advance an angled glidewire and curved catheter (e.g. C2, Kumpe, MPA) to select the TIPS and gain access to the portal system.
Exchange for a stiffer working wire and advance a pigtail flush catheter into the portal system, e.g., splenic vein.
Perform initial portal venogram to access for common issues, e.g., stenosis.
Measure portal pressure to calculate baseline HVPG. Can also measure pull back pressures across the TIPS to further localize the issue.
If revision for TIPS dysfunction/persistent/recurrent portal hypertension (e.g. variceal bleeding, ascites) -
TIPS occlusion/stenosis -> thrombolysis, thrombectomy, and/or venoplasty.
TIPS too short with pressure gradient in hepatic vein -> extend TIPS to hepatic vein ostium.
TIPS looks normal -> further dilate TIPS to 10 mm if initially 8 mm. Otherwise would need a parallel TIPS.
If revision for post-TIPS refractory hepatic encephalopathy -> TIPS reduction
Option 1: insert balloon-expandable bar metal stent parallel new smaller stent graft in hepatic vein to anchor it.
Option 2: insert balloon expandable stent and dilate to TIPS size with only the distal third out of sheath to flair and anchor the end. Carefully unsheath the rest of the stent and pull balloon back and expand proximal third creating an hour glass shape. The middle third can be dilated to a smaller diameter like 6 or 8 mm.
Option 3: insert pre-made tapered stent graft, e.g., Flare graft (Bard).
Advance pigtail catheter back into the portal system and sheath in the RA to remeasure pressures.
Post-TIP portal venogram.
Remove sheath and achieve hemostasis.
TRANSVENOUS EXTRAHEPATIC PORTOSYSTEMIC SHUNT (TEPS):
Need recent CT to carefully plan and map out anatomy.
Transabdominal technique - CT-guided puncture through the two targets, e.g., SMV and IVC with a 22G needle. Wire is snared from IJ access allowing catheterization and ultimate TEPS creation.
IVUS-guided technique - IJ + CFV or double IJ access. Often helpful for IVUS access to be lower when double IJ for better ergonomics.
Some use traditional tools. Others use a 65.5 cm 21G chiba with stylet replaced by nitrex wire and needle preloaded with 65 cm 4F CXI catheter and this placed through the metal stiffener from a Rosch Uchida set
After IVUS guided access, pullback venography performed over the nitrex to ensure track is not through a vessel or hallow viscus. Followed by TEPS creation.
For splenorenal, access achieved via 5 Fr transplenic access with Viatorr advanced via CFV access.
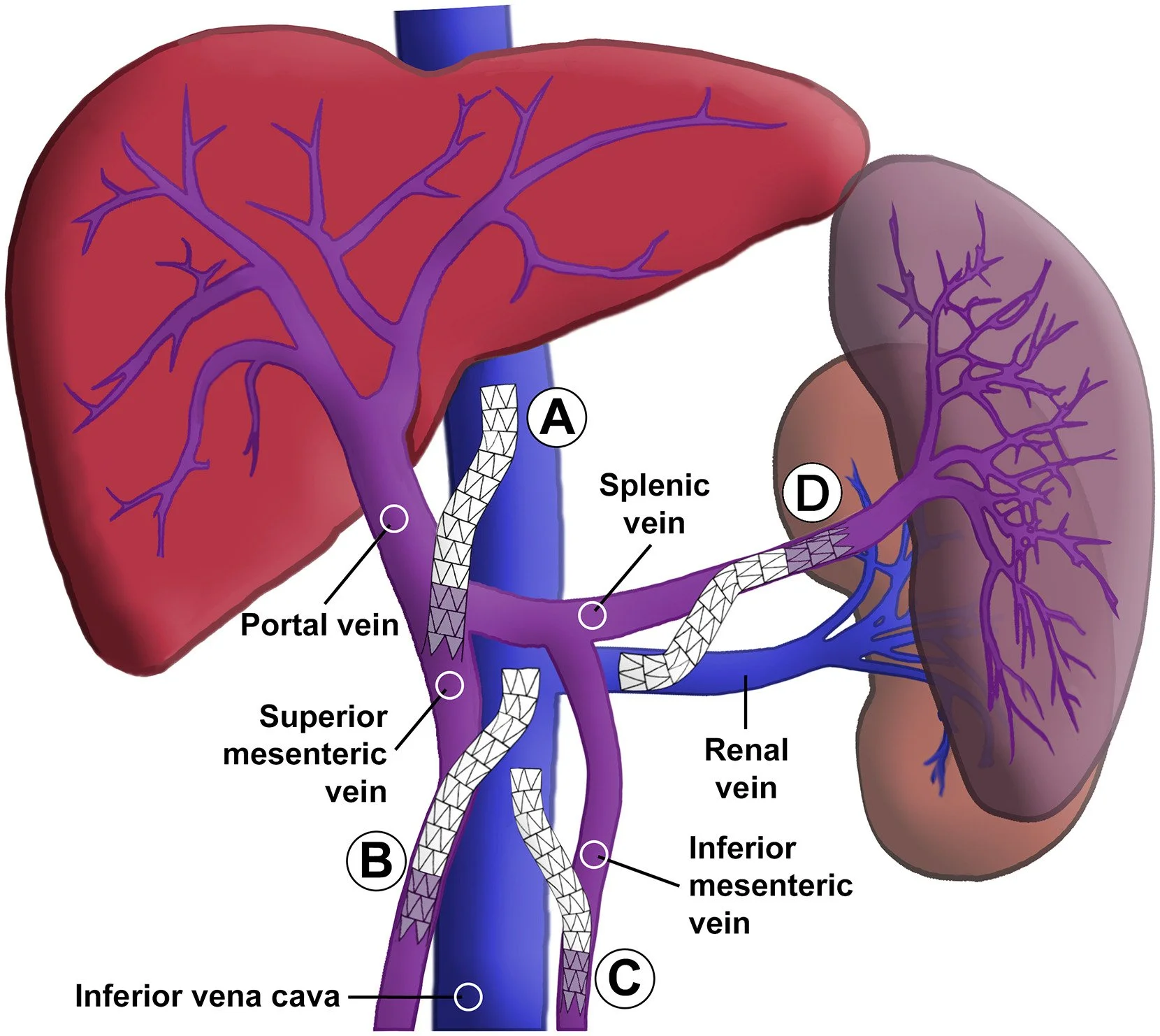
Gupta, Louie, and Sze. JVIR. 2026.
(A) Portocaval
(B) Superior mesocaval
(C) Inferior mesocaval
(D) Splenorenal
cOMPLICATIONS
Arrhythmias secondary to anesthesia or wire irritation of the endocardium while passing through the heart.
Major complications (3%): accelerated heart/liver/kidney failure, hemoperitoneum, gallbladder puncture, hemobilia, stent malposition, hepatic encephalopathy (22-50%), death
Minor complications (4%): transient AKI, hepatic artery injury, fever, jugular hematoma
Rebleeding/recurrent portal hypertension secondary to shunt stenosis or thrombosis.
Post-procedure care and follow up
Often observed overnight if not placed inpatient. Some check LFTs in first 24 hours, though some elevation is expected.
Hepatology follow up to optimize medical therapy:
Hepatic encephalopathy prophylaxis: lactulose 15g TID titrated to 2-3 bowel movements per day +/- rifaximin 550 mg BID.
Beta blocker to reduce portal hypertension: propranolol 20 mg BID or Carvedilol 12.5 mg BID for CP A and 6.25 mg BID for CP B/C.
Nutrition consult if malnourished - need 25-30 kcal/kg/d if well-compensated cirrhosis vs 30-40 kcal/kg/d if malnourished.
If TIPS placed for refractory ascites, effect can be delayed and may need a few more paracenteses.
TIPS check with doppler US, regimens vary.
Example regimen is baseline 5-10 days after placement then at 3, 6, and 12 months. Others only evaluate if clinical evidence of dysfunction.
Avoid performing in first 24 hours after placement as air within the stent graft layers can cause false positives.
TIPS dysfunction: difficult to standardize definition but should be suspected with shunt velocities <90 or >200 cm/s, change from baseline >50 cm/s, MPV velocity <30 cm/s, change in hepatofugal LPV flow (normal after TIPS) to hepatopetal.
Refractory post-TIPS hepatic encephalopathy (~7%) +/- hepatic decompensation Consider TIPS reduction or even occlusion.
Post PVR-TIPS anticoagulation if high grade PVT, slow flow at end, known pro-thrombotic disorder.