
Women's and Men's Health
Indications
Benign prostatic enlargement (BPE) with lower urinary tract symptoms (LUTS)
IPSS symptom score (7 questions) >10-13 (0-7 mild, 8-19 moderate, 20-35 severe)
BPH symptoms caused by static component of hyperplasia as well as dynamic component of sympathetic nerve stimulation causing smooth muscle contraction
QoL questionnaire >= 2
PSA <2.5 but nonspecific, if higher, should rule out prostate cancer
2.5-3.9 - consult urology for cancer risk
>4.0 probably needs a biopsy to exclude cancer
Uroflowmetry Qmax <12 mL/sec, >25 is normal, though not reliable
Prostate volume via US, CT, or MR > 40 mL
Failed trial of conservative therapy >3 months
Newer potential uses
Contraindications
Active urinary tract infection or prostatitis
Prostate cancer – can still be performed for LUTS or bleeding in collaboration with cancer treatment
Urinary obstruction due to causes other than BPH
Uncorrected coagulopathy
Relative contraindications - IPSS<12, median lobe >3cm, bladder dysfunction or cancer, prostate <50g
Efficacy and alternatives
Medications (alpha blockers and 5a reductase inhibitors) - average IPSS reduction ~3-7
Alpha blockers more effective than 5a reductase inhibitors. Combination therapy only showed benefit in larger glands.
Many sexual health complications occurring in ~15%, e.g. retrograde ejaculation
PAE - average IPSS reduction ~15
Superior to TURP in symptom relief at 1 and 3 months but equivalent at 6, 12, and 24 months
Average clinical success: 89% short term and 78% long term
Less complications and shorter recovery BUT greater symptoms recurrence
Cheaper - generally ⅓ the cost of TURP
Repeat PAE has a higher likelihood of clinical success in those who initially responded and relapsed (50-60%) vs those who never responded (20-30%)
TURP - average IPSS reduction ~15-16
Good for prostates as large as 80-100 g
Alleviates symptoms in 70%, but 18% morbidity, 50-65% ejaculatory disorders, strictures, hemorrhage, incontinence
Minimally invasive surgeries (UroLift, TUNA, Rezum, HoLEP, etc) - average IPSS reduction ~10-12
Less effective for large prostates or median lobe prominence
Generally, all minimally invasive surgical options have a 5-10 year recurrence rate
Pre-procedure work up
Some obtain CTA pelvis to characterize prostatic vascular anatomy (excellent paper on prostatic arterial anatomy)
Protocol: 800 mcg nitro 3-5 min prior to scan, 4-6 mL/s trigger 300 HU
Internal iliac artery (IIA) branching (Yamaki classification)
A (79.5%) - IIA divides into superior gluteal and common trunk for internal pudendal and inferior gluteal (“common anterior gluteal-pudendal trunk”)
B (15%) - IIA divides into internal pudendal and common gluteal trunk with small anterior division
C (5.3%) - IIA divides into superior gluteal, inferior gluteal, and internal pudendal in trifurcation
D (0.2%) - IIA divides into anterior division with common trunk for superior gluteal and internal pudendal and posterior division with inferior gluteal
Prostate Artery Origin (De Assis classification)
I (28.7%) - IIA gives off common superior and inferior vesical arteries, IVA continues as prostate artery
II (14.7%) - PA beaches directly from anterior division inferior to SVA origin; longer with fewer branches making catheterization easier
III (18.9%) - PA from upper to mid third of OA
IV (31.1%) - PA from upper to mid third of IPA
V (5.6%) - PA has other origin
Intraprostatic branching
1A - single PA with CG and PZ branches
1B - separate CG and PZ branches
2 - two communicating CG pedicles with single CG compartment
3 - two non-communicating CG pedicles with multiple CG compartments
Clinic visit with questionnaires, post void residual, PSA, UA, recent GFR
International Prostate Symptom Score (IPSS)
Quality of Life scale (QoL)
International Index of Erectile Function (IIEF)
Sexual Health Inventory for Men (SHIM)
PVR >50 mL is significant; >300 mL suggests chronic retention
Procedure steps and tips
Can insert Foley during procedure to avoid bladder filling with contrast increasing dose and obscuring anatomy, but may increase risk of urethral and median lobe trauma or UTI
Radial or femoral access -> 4/5-Fr sheath.
Inject mixture of anesthetic, vasodilator, and patient blood via 20 cc syringe for radial access
Use base catheter to select each internal iliac arteries
Radial approach: 125-cm 5-Fr Berenstein and 0.035 hydrophilic wire
Femoral approach contralateral IIA: RUC, Cobra C2, Robert’s uterine catheter (Cook), Carnevale’s prostate catheter (Merit)
Femoral approach ipsilateral IIA: RUC, Simmons I or II or same vert or Cobra 2 with Waltman loop
DSA run to map out anatomy in 20-50* ipsilateral oblique (e.g. 12 mL, 4 mL/sec)
Per Justin McWilliams (UCLA) most useful view = 45* ipsilateral oblique
Advance microwire and microcatheter system to select prostatic artery
Origin is variable (see DeAssis classification above). Tends to course lateral and then cross obturator in 97%. Often tortuous with more horizontal distal branches.
Not uncommon to have multiple, e.g, accessory prostatic branch from the IPA some call the “pena cava.” If multiple, the artery supplying the central gland is called the “arterolateral prostatic artery” and the artery supplying the periphery is called the “posterolateral prostatic artery.” There also may be supply to the seminal vesicles and ductus deferens called a vesiculodeferential artery. Embolization can effect ejaculate volume but sometimes cannot be avoided.
Common microcatheters used: ProGreat 2.4 or 2.0, Direxion 2.4, Prowler Select, 2.2-Fr Sniper with compliant balloon (Embolx)
Some data suggests balloon occlusion catheter leads to better embolization, preventing reflux and diverting flow away from distal collaterals to the low pressure prostate bed
Some perform cone beam CT prior to embolization to confirm supply and assess for collaterals
Important ones include precapsular branches with anastomosis to the IPA (“lateral accessory pudendal arteries”), penile, bladder, and rectal collaterals, which can be quite distal within the gland
Coil embolize dominant collaterals, aka skeletonize the prostate vascular supply prior to delivery. This is not always necessary with glue embolization, particularly for smaller collaterals.
Inject 100-200 ug nitroglycerin diluted in saline to prevent vasospasm or verapamil systemically. This also diverts flow away from smaller collaterals. Balloon occlusion microcatheter can have a similar effect reversing flow in collaterals towards the prostate (e.g. Sniper).
Slow embolization with dilute 300-500 micron particles diluted in 20 mL contrast via 1 mL syringe (best data). Often requires 10-15 min.
Others use 50-250 um PVA particles or glue. Study of particular distribution found that noncompressible, smaller, and more tightly calibrated particles exhibit greater distal packing.
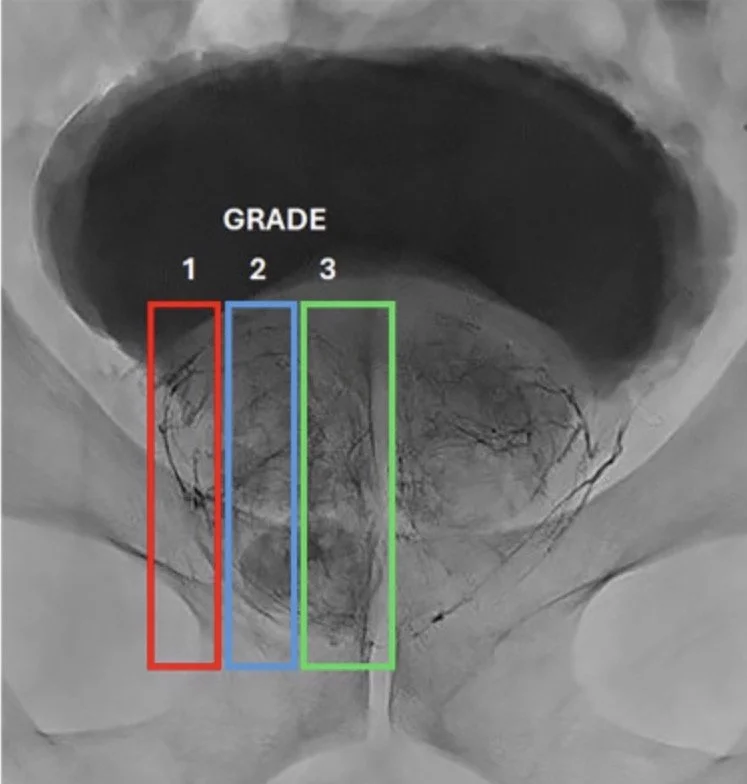
Better outcomes with glue with better penetration of the gland rated 1-3 per side with max score of 6. See picture below.
Can use PErFecTED technique where you start proximal before wedging the microcatheter into intraprostatic arteries to avoid spasm or other vascular injury, preventing embolization while attempting to get distal.
Others do the opposite of PErFecTED and get as far out as possible
Embolization target = total stasis. Important to wait 3-5 min to ensure persistent stasis.
Pull back catheter to origin of prostatic artery and perform hand run to rule out additional branches.
(Optional) Coil embolization of prostatic artery on way out (“coiling out”). Debated as this can make repeat treatment difficult without clear data-supported benefit.
Repeat process for contralateral side.
Obtain hemostasis.
Glue embolization tips - 1:10 dilute mixture of glue. Liberal use of nitroglycerine followed by deliberate steady injection. Balloon occlusion can help if available or wedging the base catheter in the origin of the prostate artery.
Complications
Clavien-Dindo grading system (I-IV): I/II = minor; III/IV = major
Minor complications / side effects: common (~60%), postembolization syndrome (10%, N/V, fever, <POD2 to 7d), dysuria (40%, <POD2 to 7d), urinary spasm/urgency (14%, <POD2 to 7d), hematuria (12%), hematospermia (16%), proctitis (6%), access site hematoma
Major complications: rare (1-5%), urinary retention (3%), UTI (2.5-4.6%), non-target embolization (e.g. bladder, rectum, and penis)
Erectile function is NOT generally affected, less retrograde ejaculation than TURP where dysfunction can occur in 10-14%. 70-89% after prostatectomy
Can prescribe PPI, steroid, prophylactic abxs, and other symptomatic medications starting 24 hrs in advance or wait until after procedure. (See after procedure section).
Post-procedure care and follow up
Optional to leave Foley 24 hrs post-PAE due to risk of urinary retention, e.g., if history of urinary retention or self catheterization
PSA can increase up to 20x 24 hours after PAE then drops to normal value (50% of baseline) at 1 month after PAE
Maintain fluid intake, restrict sexual activity, limit physical stressors such as riding bicycles or motorcycles for 1 week
Post-procedure medication regimens
Academic center:
Ibuprofen 800 mg TID
Solifenacin 5 mg
Phenazopyridine 100 mg TID
Cipro 500 mg BID for 7 days
PRN methylprednisolone DosePak (6 days) and Bisocodyl 20 mg x 7 days
Academic center:
400 mg ciprofloxacin intra-procedure, then 250 mg BID x 5 days
Phenazopyridine 100 mg TID x 5 days
Ibuprofen 800 mg TID x 5 days
Solifenacin 5 mg daily x 5 days
Anonymous OBL:
Ibuprofen 800 mg TID x 7 days - Pain
400 mg ciprofloxacin IV intra-procedure, then 500 mg BID x 7d - PPX
Pyridium 100-200 mg TID x 7 days - Burning
Oxybutynin 5 mg TID x 7 days - Bladder spasms
Docusate 100 mg BID x 7 days - Constipation
Medrol dose pack – pain
Percocet 5/325 mg, 1-2 tablets every 4-6 prn for pain
Anonymous OBL:
Ibuprofen 800 mg TID x 7 days + Medrol dose pack
Cipro 500 mg BID x 7 days
Pyridium 100-200 mg TID x 7 days
Vesicare 5 mg daily x 7 days (avoid in narrow angle glaucoma); oxybutynin as other option
Dulcolax 20 mg daily x 7 days
Continue BPH meds (e.g. alpha blocker) 1 month after to reduce risk of urinary retention
Side effects often last ~5-7 days
Urinary retention >5 hrs -> ED/urgent care
Dysuria (occurs in 60-70%) -> can double pyridium dose for 2-3 days, AZO over the counter (turns urine orange), or Uribel (turns urine blue-green)
Clinical improvement in first 2-4 weeks with peak effect at 3 months
Bladder spasms, if persistent beyond 2 weeks, consider cystoscopy